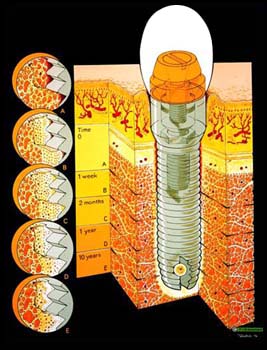
Osseointegration is the direct structural and functional connection between living bone and the surface of a load-bearing artificial implant, typically made of titanium. It is a property virtually unique to titanium, and has enhanced the science of medical bone, and
joint replacement techniques. Retention of a craniofacial
prosthesis such as an artificial ear (ear
prosthesis), eye (orbital
prosthesis), or nose (nose
prosthesis) has been practiced for a number of years; however, osseointegration of a lower
limb prosthesis is now on the horizon. Osseointegration in humans was discovered in 1952 during animal experiments and has been used for lower
limb prostheses since the 1990s.
The first
amputee to undergo this procedure was a very high level bilateral above knee
amputee, who was not an ideal candidate for conventional prostheses. At accomplish this, titanium bolts, called “abutments” were attached to the
distal ends of both femur bones. The prosthetic knee and foot components attach directly to these bolts. This procedure involves two major surgeries, the first to thread the device into the skeleton and the second to re-expose the fixture and attach the bolt. Both surgeries involve extended recoveries, with an estimated six month recovery for each surgery. Approximately 100 lower
limb and 30 upper
limb amputees have undergone this procedure.
The main advantages of osseointegration, over conventional prosthetic fittings, are:
· The
prosthesis feel more like a natural extension of the human body, with no artificial
interface
· Less components mean the
prosthesis is lighter weight
· The user reports better control over the
prosthesis
All problems associated with prosthetic sockets, including discomfort, sweating, volume change and skin breakdown, are eliminated as this design does not incorporate a prosthetic
socket The procedure, however, is not without its faults:
· The user must undergo two surgeries, which both pose health risks
· Long surgery recovery
· Delay of prosthetic fitting, which is normally recommended soon after
amputation, for the user’s emotional and physical health
· There is a high risk of infection as the bolt extending from the femur is essentially a permanently open wound
· Possibility of bone fracture due to excessive weight load
· The fixture can become unthreaded from the bone and detach from the user
The
socket is often the most problematic
component of a
prosthesis, as it is in constant contact with the
residual limb and is commonly the source of discomfort for an
amputee. Osseointegration eliminates the
socket, but also eliminates the most important function of a lower
limb prosthetic
socket. For lower
limb amputees, particularly above knee amputees, an ischial containment
socket locks onto the pelvis and ensures ultimate stability during
ambulation. It provides greater distribution of pressure and stress throughout multiple areas of the body.
With osseointegration, 100% of the pressure and stress is focused at the
distal end of the femur. The osseointegration fixture is designed to pull muscle away from the
distal end of the bone, thereby limiting movement of skin around the bolt site. This makes it more difficult for bacteria to enter the site and grow. If bacteria do form, antibiotics are used. Serious infection could lead to
revision surgery and even a higher level of
amputation. Despite the huge risk factor involved in this procedure, it is no doubt the logical conclusion in prosthetic technological developments.