Ankle-foot orthosis (abbreviated: AFO) is a brace, usually plastic, worn on the lower leg and foot to support the ankle, hold the foot and ankle in the correct position, and correct foot drop. Also known as a foot-drop brace. AFOs are commonly used in the treatment of disorders that affect muscle function such as stroke, spinal cord injury, muscular dystrophy, cerebral palsy, polio and multiple sclerosis. AFOs can be used either by providing support to weak or wasted limbs or by positioning a limb with tight, contracted muscles into a more normal position. AFOs are also used to immobilize the ankle and lower leg in the presence of arthritis or fracture.
AFOs
The method of obtaining a good fit with an AFO involves one of 2 approaches:
1. provision of an off-the-shelf or prefabricated AFO matched in size to the end user
2. Custom manufacture of an individualized AFO from a positive model obtaining by means of a negative cast or the use of computer assisted imaging, design, and milling. The plastic used to create a durable AFO must be heated to +/- 400 degrees Fahrenheit, making direct molding of the material to the end user impossible.
AFO's generally refer to lightweight ploypropylene based plastic braces. The devices are attached to the calf with a strap and a piece runs up under the foot, fitting inside an accomodative shoe. The "L" effect of the plastic shell counteracts foot drop and allows those suffering to better control their movement. The use of generic descriptions of orthopedic braces, such as ankle foot orthosis, began in the late 1970s as the result of work done by the American Academy of Orthopedic Surgeon in order to make classification of such braces easy. The initial description in the literature of the device now referred to as an ankle foot orthosis was made by York, et al in the late 1960s. Prior to that time, braces that affected the lower leg were limited to metal and leather designs attached to the shoe or plaster casts, called short leg braces or short leg casts.
The effects of an ankle-foot orthosis (AFO) on ankle and knee biomechanics during walking.
Therapists often recommend, and physicians frequently prescribe the ankle-foot orthosis (AFO) for patients with gait deviations that relate to muscle weakness. The AFO substitutes for weak dorsiflexors during swing and, more importantly, for weak plantar flexors during stance.
The AFO's effect on supporting the forefoot and preventing plantar flexion or "foot drop" during swing is straightforward. Less obvious is the AFO's role as a substitute for plantar flexor muscles. The plantar flexors must be active during midstance and terminal stance to counter the dorsiflexor moment that is produced by the ground reaction force. If the plantar flexors are weak, the ankle dorsiflexes too rapidly and, because the lower extremity is positioned in a closed chain, the knee flexes.
Midstance knee flexion threatens the person's stability. Someone with weak plantar flexors must compensate, or must wear an external device (an orthosis) that substitutes the force that the plantar flexors ordinarily provide.
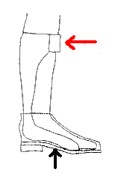
When a person bears weight on an AFO that he or she wears inside the shoe, the AFO's rigid walls transfer the ground reaction force (black arrow) in the direction indicated by the red arrow. Thus, the AFO directs a force posteriorly against the anterior tibia during midstance and terminal stance, and prevents or controls tibial advancement. In this way, the AFO's force produces a plantar flexion moment that counters the ground reaction force's (GRF) tendency to dorsiflex the ankle.
The AFO's ability to redirect the ground reaction force, and thereby produce a plantar flexor moment, depends on its rigidity. An AFO that is flexible or articulated (hinged at the ankle) does not serve this purpose.
In addition to producing a force that pushes posteriorly on the tibia, in the direction of ankle plantar flexion, an AFO can influence the ground reaction force's effect on the knee.
• If the orthotist aligns the AFO in plantar flexion, the alignment inclines the tibia posteriorly during stance. This ankle alignment causes the knee joint's lateral axis to lie more posteriorly. In this location, the knee joint axis lies posterior to the ground reaction force's line of application throughout a longer period of time during the walking cycle. Therefore, this plantar flexed alignment increases the time during which the ground reaction force lies anterior to the knee joint axis, and produces knee extension.
The diagram illustrates an AFO that is aligned in five degrees of plantar flexion.
• Alternatively, when the orthotist aligns the AFO in dorsiflexion, the tibia is inclined more anteriorly during stance. This tibial position causes the knee joint axis to lie further anterior, and increases the period of time during which the ground reaction force lies posterior to the knee joint axis, and produces knee flexion.

The diagram illustrates an AFO that is aligned in five degrees of dorsiflexion.